What causes young-onset dementia?
The causes of young-onset dementia, also known as early-onset dementia, are different from those in older people. The young-onset of some of the most common types of dementia are described on this page.
Young-onset dementia
What are the causes of young-onset dementia?
The causes of young-onset, or early-onset dementia are similar to the diseases that usually cause dementia in older people. However, some causes, such as frontotemporal dementia (FTD), are more common in younger people. Dementia in younger people often has different symptoms, even when it’s caused by the same diseases as in older people.
There is more information about some common causes of dementia, and how they can affect younger people, below.
Alzheimer’s disease
Alzheimer's disease is the most common type of early-onset dementia and may affect around 1 in 3 younger people with dementia. However, up to 2 in 3 older people with dementia have Alzheimer’s disease. Alzheimer’s disease develops when proteins build up in the brain to form structures called ‘plaques’ and ‘tangles’. This causes brain cells to die and so affects functions controlled by the brain.
For most older people with Alzheimer’s disease, the first symptom they notice is likely to be memory loss. However, in younger people with Alzheimer’s disease, memory loss is less likely to be the first symptom.
Atypical Alzheimer’s disease
Younger people are much more likely to have an ‘atypical’ (unusual) form of Alzheimer’s disease. The symptoms depend on the specific form a person has:
- In posterior cortical atrophy (PCA) the first symptoms are usually problems with understanding visual information, such as struggling to read or judge distances.
- In logopenic aphasia the first symptoms are usually difficulties with language, such as problems finding the right word, or taking long pauses while they speak.
- In behavioural/dysexecutive Alzheimer’s disease the first symptoms are usually difficulties with planning and decision making, and behaving in socially inappropriate ways.
Up to 1 in 3 younger people with Alzheimer’s disease have one of these forms, but only 1 in 20 older people with Alzheimer’s disease have an atypical form. For more information see Rarer types of dementia.
Familial Alzheimer's disease
Familial Alzheimer’s disease is a very rare form of Alzheimer’s disease. It is caused by genetic mutations (changes in genes) that run in families. Three genes have been found to have these rare mutations – PSEN1 (presenilin 1), PSEN2 (presenilin 2) and APP (amyloid precursor protein).
There is a 50% risk of a parent passing on the familial Alzheimer’s disease mutation to their children. People with the condition usually have a strong family history of the disease and will know a range of family members who were affected at a similar age, along with one of their parents.
Symptoms of familial Alzheimer’s disease usually start in someone’s 30s, 40s or 50s. The earlier the symptoms start, the more likely it is that the disease is genetic. Familial Alzheimer’s disease is very rare and probably accounts for fewer than 1 in 100 people with Alzheimer’s disease. For more information see Types of genetic testing.
Learning disabilities and dementia
People with Down’s syndrome and other learning disabilities are more likely to develop dementia when they are younger. Dementia in people with Down’s syndrome is usually caused by Alzheimer’s disease, but not always.
The reasons why people with Down’s syndrome are at increased risk of Alzheimer’s disease are not well understood. It is thought to be due to chromosome 21, which most people with Down’s syndrome have an extra copy of. This leads to an overdevelopment of a protein (amyloid precursor protein) which forms plaques on the brain. These plaques are a feature of Alzheimer’s disease. By the age of about 40, almost all people with Down’s syndrome have changes in the frontal lobe of their brain. However, not everyone will develop the symptoms of dementia.
Learning disabilities and dementia
Read more about why someone with a learning disability is more likely to develop dementia and the ways in which they can be supported to live well with the condition.
Vascular dementia
Vascular dementia is caused by problems in the blood supply to the brain. It is closely linked to diabetes and to cardiovascular diseases such as stroke and heart disease.
Symptoms of vascular dementia vary from person to person. Early memory loss is less common. However, other symptoms are more common in vascular dementia, including slower speed of thought and problems with:
- planning
- organising
- making decisions
- solving problems
- following a series of steps
- concentrating.
Physical symptoms (such as limb weakness) are common in vascular dementia when a person develops it after a stroke.
For more, see What is vascular dementia?
CADASIL
CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy) is a rare genetic form of vascular dementia. It is a disease of the blood vessels in the brain. Symptoms include migraines and repeated strokes, loss of mental abilities, seizures, apathy and depression. They usually start when a person is in their mid 30s.
CADASIL is caused by a genetic mutation in the NOTCH3 gene. It is usually inherited from a parent who has a 50% chance of passing on the mutated copy of the gene.
For more information see Rarer types of dementia.
Frontotemporal dementia
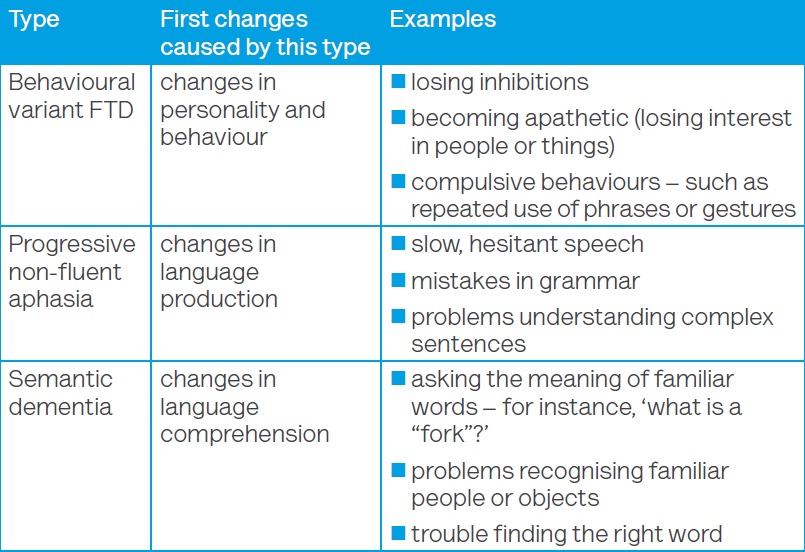
Frontotemporal dementia is caused by damage to the lobes at the front and/or sides of the brain. It is much more common in younger people with dementia than in older people. FTD is most often diagnosed in people between the ages of 45 and 65. This is different to Alzheimer’s disease, vascular dementia and dementia with Lewy bodies, which all become more likely as people get older. There are three different types of FTD which cause different changes as the first symptoms.
For more information see Frontotemporal dementia: what is it?
Is FTD inherited?
About 20–40% of people with FTD have a family history of dementia. About 10% of people with FTD have a strong family history, with several close relatives from different generations affected.
The three main mutations causing FTD are in the progranulin (GRN), microtubule-associated protein tau (MAPT) and chromosome 9 open reading frame 72 (C9ORF72) genes.
The children or siblings of someone with a genetic mutation known to cause FTD have a 50% chance of carrying the same mutation. Families with a known mutation should be offered genetic counselling.
For more information see Genetics of dementia.
Dementia with Lewy bodies (DLB)
Dementia with Lewy bodies is caused by the build-up of tiny protein deposits (Lewy bodies) in the brain. DLB is less common in younger people with dementia than in older people. Lewy bodies also cause Parkinson’s disease and about one-third of people with Parkinson’s eventually develop dementia.
Symptoms of dementia with Lewy bodies can include hallucinations and varying levels of alertness. People can also develop the features of Parkinson’s disease (such as slower movement, stiffness and trembling limbs).
What is dementia with Lewy bodies?
Find out more about dementia with Lewy bodies, diagnosis and how to treat it.
Alcohol-related brain damage
Alcohol-related brain damage is caused by regularly drinking too much alcohol over several years. It covers a range of conditions including alcohol-related dementia and Wernicke–Korsakoff syndrome. People diagnosed with ARBD tend to be in their 40s and 50s, and it is more common in men.
ARBD is caused by a lack of thiamine (vitamin B1), direct damage to nerve cells from alcohol, head injuries (caused for instance by falls or fights) and a poor diet.
At least 1 in 10 younger people with dementia may have ARBD. Symptoms will depend on the cause of the ARBD. They can include problems with planning, organising, problem solving, attention and controlling emotions. They can also include changes in personality, difficulties learning new skills and disorientation.
Many people diagnosed with ARBD who stop drinking alcohol and receive good support (including treatment and a good diet) can see improvement in their symptoms. Sometimes they can make a partial, if not full, recovery.
For more information see Alcohol-related brain damage.
Rarer causes of dementia
Rarer causes of dementia are more common in younger people than in older people. There are also a range of conditions that can cause symptoms similar to dementia in younger people.
For more information on these types of dementia see Rarer types of dementia.
Genetic testing
People who are at increased risk of a genetic mutation that causes dementia should be offered genetic testing.
There are two types of genetic testing:
- diagnostic genetic testing – for people with a diagnosis and a strong family history of dementia
- predictive genetic testing – for people without symptoms but who have a high risk of inheriting dementia.
Before the genetic testing, the person and their family should be offered genetic counselling. This should explain the process and how it could affect them and should be offered for several months before and after the genetic testing. The person and their family will be asked if they want to know the outcome or have it kept on file for a later date. It’s important that the person and their family agree together as the decision will affect the whole family. Many people choose not to go ahead with the genetic testing after counselling, but it is up to each person to make the right decision for them.
A person should consider carefully whether they want genetic testing. There are both advantages and disadvantages to knowing whether they have a genetic mutation. Some people want to find out because it means they know they are carrying a mutation and it can remove the uncertainty. It can also mean they can take it into account when planning their future – for instance, if they’re considering having children. For some people it leads to taking part in research into dementia too.
However, there are disadvantages as well. It can lead to feelings of guilt, especially related to other family members. Knowing there is a genetic mutation can cause depression, grief and anger for some people, as they are living with the knowledge that they will almost certainly develop dementia. It can also cause a lot of stress if people spend a lot of time ‘looking’ for symptoms.
Deciding whether or not to go ahead with genetic testing is a very personal decision and it is important that people receive support from trained professionals to help them with the process.
For more about genetic testing see Genetics of dementia.





